根据9月21日发表于JAMA杂志的一项前瞻性、观察性研究报告显示,血小板功能检测中显示氯吡格雷负荷后残留高血小板反应性的急性冠脉综合征(ACS)患者短期和长期缺血性事件风险增高。
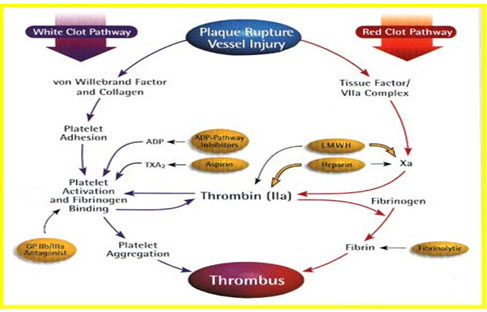
急性冠脉综合征成因
为了评估氯吡格雷负荷后残留血小板反应性能否作为一种预后标志物,意大利佛罗伦萨市Careggi医院心内科的Guido Parodi医生及其合作者对4年期间在该中心接受经皮冠脉介入治疗(PCI)+支架置入的连续1,789例ACS患者进行了一项前瞻性、观察性、队列研究。在给予600mg负荷剂量氯吡格雷后12~18 h使用透光率集合度检测方法与二磷酸腺苷(ADP)激动剂测定血小板反应性。ADP检测中残留高血小板反应性的总发生率为14%,研究者认为该结果偏低。主要终点为在随访2年期间发生缺血性事件的复合终点,包括心源性死亡、心肌梗死、紧急冠脉血运重建和卒中。
结果显示,残留高血小板反应性者的主要终点发生率为14.6%,而其他患者仅为8.7%。“主要终点事件发生率的差异主要受到心源性死亡率的影响,残留高血小板反应性组中患者的心源性死亡率为9.7%,而残留低血小板反应性组仅为4.3%,两组患者其他主要终点构成部分的发生率无差异”(JAMA 2011;306:1215-23)。基线后6个月内即可观察到心源性死亡率增高,并持续至随访结束。残留高血小板反应性者的次要终点——支架内血栓形成的发生率为其他患者的2倍(6.1% vs. 2.9%)。
最初显示氯吡格雷负荷后高血小板反应性的患者接受了干预。在ADP指导下增加氯吡格雷维持剂量或在ADP指导下转为噻氯匹定治疗,使该组62%的患者的血小板反应性恢复正常,其余38%的患者仍显示持续高血小板反应性,但这两个亚组患者的预后无统计学差异。
研究者总结认为,上述研究结果支持氯吡格雷负荷后残留高血小板反应性是缺血性事件预测标志物的假设,且血小板反应性正常化并不能使预后改善。
生物探索推荐论文摘要:
High Residual Platelet Reactivity After Clopidogrel Loading and Long-term Cardiovascular Events Among Patients With Acute Coronary Syndromes Undergoing PCI
Context High residual platelet reactivity (HRPR) in patients receiving clopidogrel has been associated with high risk of ischemic events after percutaneous coronary intervention (PCI).
Objective To test the hypothesis that HRPR after clopidogrel loading is an independent prognostic marker of risk of long-term thrombotic events in patients with acute coronary syndromes (ACS) undergoing an invasive procedure and antithrombotic treatment adjusted according to the results of platelet function tests.
Design, Setting, and Patients Prospective, observational, referral center cohort study of 1789 consecutive patients with ACS undergoing PCI from April 2005 to April 2009 at the Division of Cardiology of Careggi Hospital, Florence, Italy, in whom platelet reactivity was prospectively assessed by light transmittance aggregometry.
Interventions All patients received 325 mg of aspirin and a loading dose of 600 mg of clopidogrel followed by a maintenance dosage of 325 mg/d of aspirin and 75 mg/d of clopidogrel for at least 6 months. Patients with HRPR as assessed by adenosine diphosphate test (≥70% platelet aggregation) received an increased dose of clopidogrel (150-300 mg/d) or switched to ticlopidine (500-1000 mg/d) under adenosine diphosphate test guidance.
Main Outcome Measures The primary end point was a composite of cardiac death, myocardial infarction, any urgent coronary revascularization, and stroke at 2-year follow-up. Secondary end points were stent thrombosis and each component of the primary end point.
Results The primary end point event rate was 14.6% (36/247) in patients with HRPR and 8.7% (132/1525) in patients with low residual platelet reactivity (absolute risk increase, 5.9%; 95% CI, 1.6%-11.1%; P = .003). Stent thrombosis was higher in the HRPR group compared with the low residual platelet reactivity group (6.1% [15/247] vs 2.9% [44/1525]; absolute risk increase, 3.2%; 95% CI, 0.4%-6.7%; P = .01). By multivariable analysis, HRPR was independently associated with the primary end point (hazard ratio, 1.49; 95% CI, 1.08-2.05; P = .02) and with cardiac mortality (hazard ratio, 1.81; 95% CI, 1.18-2.76; P = .006).
Conclusion Among patients receiving platelet reactivity–guided antithrombotic medication after PCI, HRPR status was significantly associated with increased risk of ischemic events at short- and long-term follow-up.






