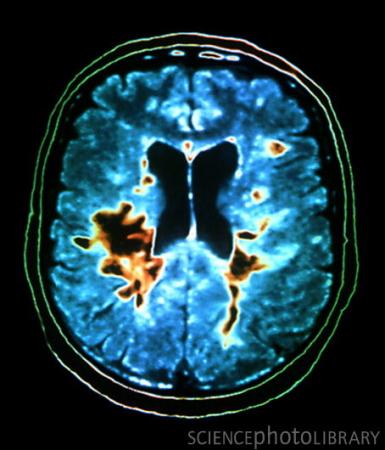
多发性硬化症患者的脑部CT扫描(图)
英国科学家们最近发现了新的和多发性硬化症相关的29种突变基因,为未来新药物的研发提供了更完善的理论依据。
多发性硬化(multiple sclerosis,MS)是一种中枢神经系统脱髓鞘疾病,青、中年多见,临床特点是病灶播散广泛,病程中常有缓解复发的神经系统损害症状。 该病的病变位于脑部或脊髓。神经细胞有许多树枝状的神经纤维,这些纤维就像错综复杂的电线一般。多发性硬化症就是因为在中枢神经系统中产生大小不一的块状髓鞘脱失而产生症状。所谓“硬化”指的是这些髓鞘脱失的区域因为组织修复的过程中产生的疤痕组织而变硬。这些硬块可能会有好几个,随着时间的进展,新的硬块也可能出现,所以称作“多发性”。
多发性硬化症的初期不易被检查出来。如视力模糊或复视等,常见的症状有一定部位的肌肉僵硬,乏力、丧失控制能力,四肢异常疲劳、行走困难,头晕,膀胱控制失调,触觉、痛觉和温热感觉紊乱等,每个症状出现后又会消失。就这样一个接一个的相继发生,或继续恶化,最后可使患者吞咽困难。致残及卧床不起。还没有治疗这种疾病的特效药物。
这项研究的论文发表在最新一期的《Nature》杂志上。科学家们研究证实了T细胞和白细胞介素对该疾病的形成至关重要,
为了这项研究,牛津大学的Compston 和Peter Donnelly,以及他们的250位同事,研究了9772例患有多发性硬化病人的基因,并与超过17300例正常人的基因进行比较。研究分析结果显示,除了之前研究已经确认的23个于疾病发生相关的基因突变外,它们还发现了29个新的基因突变。
目前研发的靶向人体免疫系统的药物包括有rituximab(用于治疗白血病)、Tysabri、Lemtrada(用于治疗癌症)、Zenapax和daclizumab等等。
论文的通讯作者,英国剑桥大学的Alastair Compston说道:“我们证实了多发性硬化症属于免疫系统疾病,并且检测了所有对上诉药物会起反应的基因,这将有助于未来的治疗。”
在另一篇发表在《PLoS Genetics》杂志的论文指出,许多和多发性硬化发生相关的基因与其它的一些免疫性疾病也相关,如节段型肠炎和I型糖尿病。这说明目前的这些药物还有治疗其它疾病的潜在功能。
《PLoS》论文的主要作者,美国耶鲁大学的Chris Cotsapas说道:“我们推测与免疫系统相关的一些重大疾病应当和一些常见的基因突变有关,通过这项研究,我们找到了未来治疗的靶点。”
之前也有研究证实维生素D不足的人可能患有多发性硬化症的风险较高。在Compston发现的这些基因里,也包括有两种和维生素D代谢相关的基因。(生物探索 Jun译)
生物探索推荐英文论文原文摘要:
Genetic risk and a primary role for cell-mediated immune mechanisms in multiple sclerosis
Multiple sclerosis is a common disease of the central nervous system in which the interplay between inflammatory and neurodegenerative processes typically results in intermittent neurological disturbance followed by progressive accumulation of disability. Epidemiological studies have shown that genetic factors are primarily responsible for the substantially increased frequency of the disease seen in the relatives of affected individuals and systematic attempts to identify linkage in multiplex families have confirmed that variation within the major histocompatibility complex (MHC) exerts the greatest individual effect on risk. Modestly powered genome-wide association studies (GWAS) have enabled more than 20 additional risk loci to be identified and have shown that multiple variants exerting modest individual effects have a key role in disease susceptibility. Most of the genetic architecture underlying susceptibility to the disease remains to be defined and is anticipated to require the analysis of sample sizes that are beyond the numbers currently available to individual research groups. In a collaborative GWAS involving 9,772 cases of European descent collected by 23 research groups working in 15 different countries, we have replicated almost all of the previously suggested associations and identified at least a further 29 novel susceptibility loci. Within the MHC we have refined the identity of the HLA-DRB1 risk alleles and confirmed that variation in the HLA-A gene underlies the independent protective effect attributable to the class I region. Immunologically relevant genes are significantly overrepresented among those mapping close to the identified loci and particularly implicate T-helper-cell differentiation in the pathogenesis of multiple sclerosis.






